Today’s case is presented by Dr. Jordan Friedmann, a PGY3 Internal Medicine Resident. He walks us through a case that involves many different opinions and treatment path options. The group examines how crucial the advise of many disciplines can be and the importance of owning your case as the most responsible physician.
ID –
56yo active male, presenting with 4wk hx of abdominal pain and fatigue
HPI –
Epigastric pain consistent with previous reflux
Post-prandial lower abdominal cramping
Recent weight loss, subjective fever, chills
No vomiting, diarrhea, night sweats
Negative ROS
PMHx –
Membranous nephropathy – kidney transplant in youth from sister, baseline Cr 130s
Asthma – well-controlled
Osteoarthritis in knees
Mild prostatic hypertrophy
GERD
Medications –
Azathioprine 25mg daily – not totally compliant
Cyclosporine 50mg BID
Ventolin puffer prn
Family Hx –
Sister has mild lupus
Social Hx –
Plays many sports
Works in software
Lives locally with roommate
No family or kids
Born in India, but grew up in Canada
Extensive world traveller – has been to Eastern Europe, Thailand, and Bali in last 5 yrs
No drugs or alcohol use
Initial Investigations
- Investigations
- Blood
- WBC 14 × 109/L (normal 3.5 – 10.5 x 109/L)
- Eosinophils 5.1 × 109/L (normal 0 – 0.5 x 109/L)
- Hgb 135 g/L (normal 125-170 g/L)
- Plt 470 × 109/L (normal 130 – 380 x 109/L)
- Electrolytes normal, renal function baseline
- CRP 32 mg/L (normal ≤ 10 mg/L)
- Urine
- Urinalysis bland
- Imaging
- CT abdo – Enteritis of small bowel. Differential includes infectious or inflammatory causes with ischemia less likely. No arterial or venous abnormality. Graft vs. host disease is a possibility
- Blood
Discussion #1 – Broad differential

More information
- Investigations
- Blood
- Eosinophils 5.1 × 109/L -> 10 × 109/L (normal 0 – 0.5 x 109/L)
- IgE 1500 (ULN 500)
- ANCA negative, SPEP negative
- AM cortisol normal
- B12 normal
- Infectious
- HIV, CMV, Hep B/C, EBV serologies negative
- Syphilis negative
- Ova and parasites negative but Charcot-Leyden crystals seen
- Endoscopy
- Upper endoscopy – hiatal hernia, biopsies taken
- Lower endoscopy – no lesions, biopsies taken
- Blood
Discussion #2 – Strongyloidiasis1
- Caused by Strongyloides stercoralis, a common intestinal nematode
- Epidemiology
- Endemic in Africa, Asia, Southeast Asia, and Central and South America
- Infection occurs when infective larvae penetrate intact skin, most commonly when bare feet come in direct contact with contaminated soil
- Can have long asymptomatic period
- Clinical features
- Gastrointestinal most common
- Progressive weight loss, diarrhea, abdominal pain, vomiting
- Dermatologic
- Larva currens – pruritic, linear rash in lower trunk, perianal regions
- Additional features in immunosuppressed hosts that may indicate dissemination
- Fever
- Gram-negative/polymicrobial bacteremia from larvae migration through bowel wall
- Respiratory
- Dyspnea, wheeze, hemoptysis, cough, respiratory distress
- Gastrointestinal most common
- Diagnosis
- If stable and no features or risk factors of disseminated disease, screen 3 serial stool samples for ova and parasites and ELISA test
- If unwell and features or risk factors of disseminated disease, obtain blood and sputum cultures +/- CSF in addition to above
- Should be recognized before initiating corticosteroid therapy which could have catastrophic effects in strongyloidiasis
More information
- Investigations before discharge
- Blood
- Eosinophils 5.1 × 109/L -> 10 × 109/L -> Peak 2 days after receiving Ivermectin -> 5.6 × 109/L (normal 0 – 0.5 x 109/L)
- Infectious
- Schistosomiasis negative
- Imaging
- MR enterogram – interval improvement
- Blood
- Investigations as outpatient 1 week after discharge
- Blood
- Eosinophils 4.2 × 109/L (normal 0 – 0.5 x 109/L)
- Blood
- Investigations as inpatient after readmission with abdominal pain
- Infectious
- Strongyloides serology negative
- Pathology
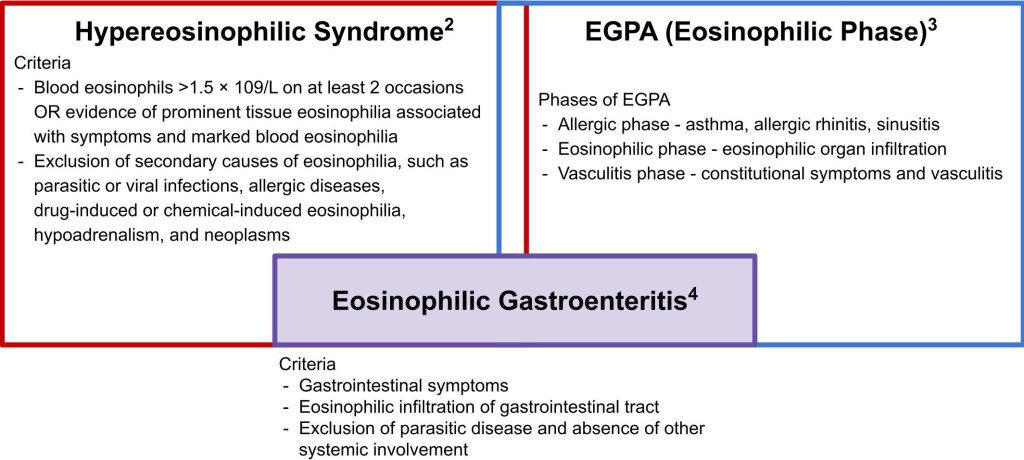
- Colon biopsy – Focal submucosal non-necrotizing granuloma. No vasculitis seen. No myobacterial organisms. Eosinophilic inflammation of submucosa. Differential includes eosinophilic enteritis, parasitic infection, systemic hypereosinophilic syndrome, and EGPA. Not consistent with IBD.
- Infectious
Discussion #3 – Narrowing the differential

More information
- Investigations
- Blood
- Flow cytometry on peripheral blood – normal
- Tryptase normal
- IgG4 ~10 g/L (0.052–1.250 g/L)
- Pathology
- Colon biopsy – IgG4 staining negative
- Blood
Discussion #4 – IgG4 elevation
Please refer to S5 E14 shownotes discussion #3 for a differential of IgG4 elevation beyond IgG4-related disease and results of a study by Carruthers et al. noting it’s modest PPV of 34% for IgG4-related disease.
https://stpaulsmorningreport.com/2021/08/07/s5-e14-snowball/
More information
- Investigations
- Pathology
- Colon biopsy – Thought to be consistent with EGPA
- Pathology
Discussion #5 – Overlap in diagnosis
References
- Lim S, Katz K, Krajden S, Fuksa M, Keystone JS, Kain KC. Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management. CMAJ. 2004 Aug 31;171(5):479–84.
- Simon H-U, Rothenberg ME, Bochner BS, Weller PF, Wardlaw AJ, Wechsler ME, et al. Refining the definition of hypereosinophilic syndrome. J Allergy Clin Immunol. 2010 Jul;126(1):45–9.
- Gioffredi A, Maritati F, Oliva E, Buzio C. Eosinophilic Granulomatosis with Polyangiitis: An Overview. Front Immunol. 2014 Nov 3;5:549.
- Ingle SB, Hinge (Ingle) CR. Eosinophilic gastroenteritis: An unusual type of gastroenteritis. World J Gastroenterol. 2013 Aug 21;19(31):5061–6.
