Join us as we watch a simple case snowball into a hard one. And this time it’s not our fault!
ID –
64 year old male, hx of insulin-dependent T2DM, CAD, untreated HepC, presenting with upper GI bleed.
HPI –
Sept 2019 – New onset chest and diffuse abdominal pain. No records available. Received dx of some “rare pancreatic cancer.” Treated with prednisone, but rapidly developed cushingoid features. Discontinued prednisone. Lost to follow-up and moved to BC.
A month later – Admitted to hospital with upper GI bleed. H pylori positive. Admission complicated by DKA. Abdominal pain with CT abdo demonstrating ill-defined hypodensity in pancreatic head, slight cyst draining in adjacent mesentary, prominence of common bile duct, could represent acute pancreatitis. Non-opacification of splenic vein in keeping with splenic vein thrombosis.
PMHx –
T2DM – Insulin dependent, peripheral neuropathy, last A1c 8.6%
CAD – PCI to LAD in 2015
Hep C – untreated
HTN
Medications –
Rosuvastatin
Rabeprazole
Aspirin
Ramipril
Insulin
Social Hx –
Works as a chef
Light smoker, minimal alcohol, regular cannabis user
Allergies –
No known allergies
Discussion #1 @4:35 – Creating a problem list
1. DKA
- Potential triggers
- Upper GI bleed
- Prednisone
- Pancreatitis
2. Splenic vein thrombosis
- Differential
- Cirrhosis
- Malignancy
- IBD
- Pancreatitis
- Inherited clotting disorders
- Abdominal surgery
3. Untreated HepC
- Relevant extra-hepatic manifestations
- Cryoglobulinemia
- Autoimmune hepatitis
More Information
- Discharged without unifying diagnosis after acute UGIB and DKA managed
- Only remaining symptom is ongoing vomiting
- Aug. 2020 – admission following bike accident with severe bruising
- Investigations
- Imaging
- CT abdomen and pelvis – Mildly edematous-appearing pancreas with peripancreatic fat stranding suggesting acute pancreatitis. Common bile duct dilated up to 1cm with suspected wall thickening distally and appearance similar to Nov. 2019. Subtle non-specific areas of wedge-shaped hypoattenuation in both kidneys. Splenic vein thrombosis persists.
- Bloodwork
- Normal CBC
- Normal renal function
- Lipase 76 IU/L, ALT 60 IU/L, AST 41 IU/L, ALP 189 IU/L, GGT 98 IU/L, albumin 28 g/L, total bili 6 µmol/L
- HepB negative, non-immune
- HCV viral load 145,000, genotype 1A
- Imaging
- Investigations
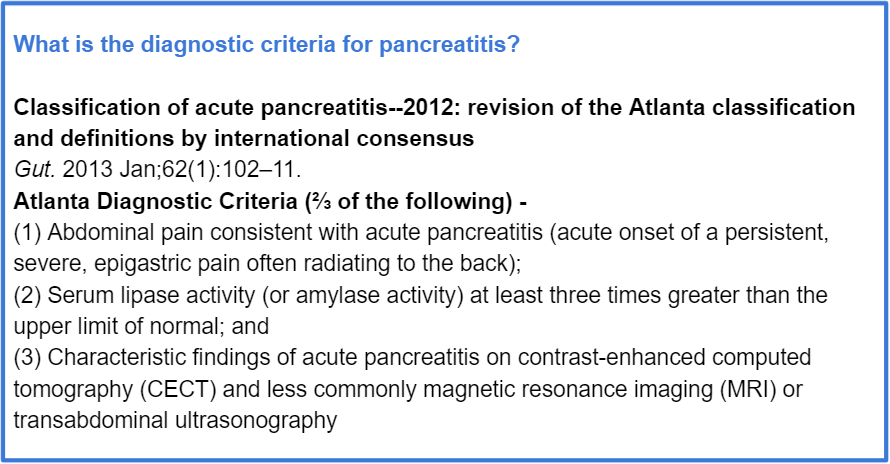
Discussion #2 @17:58 – Is this pancreatitis?
More information
- Oral and ocular sicca on history
- Investigations
- Bloodwork
- Hgb 121 g/L, WBC 7×109/L, Plt 146×109/L
- Normal calcium
- Normal triglycerides
- Total bili 6 µmol/L, ALT 45 IU/L, ALP 129 IU/L, GGT 125 IU/L
- Creatinine 85 µmol/L, eGFR 84
- C3 0.45, C4 unmeasurably low, ANA/EMA/AMA negative
- Imaging
- CT chest, abdo, and pelvis
- Several scattered nodules bilaterally throughout the lungs. Chronic sausage pancreas with hypodensity halo and several peripancreatic and paracaval lymph nodes, no pseudocysts. Slight increase in circumferential wall thickening of common bile duct and associated narrowing of the lumen, stable intrahepatic biliary duct dilatation. Bilateral renal wedge-shaped hypodensities, chronic splenic vein thrombosis, and narrowing of portal confluence.
- Bloodwork
Discussion #3 @26:56 – Differential diagnosis
| Factors For | Factors Against | |
| 1. IgG4-Related Disease | – Characteristic radiologic appearance of pancreas – Renal hypodensities – Previously treated with prednisone – Sicca – Multiorgan involvement – Decreased C3/C4 | |
| 2. Sarcoidosis | – Lung nodules – Sicca – Multiorgan involvement – Decreased C3/C4 | – Very rarely involves pancreas |
| 3. Castleman’s Disease | – Lung nodules – Multiorgan involvement – Decreased C3/C4 | – Lacking constitutional symptoms – Rarely involves pancreas |
More information
- Investigations
- Bloodwork
- IgG 29 g/L
- IgG4 1.5 g/L previously -> 10.2 g/L now
- Bloodwork
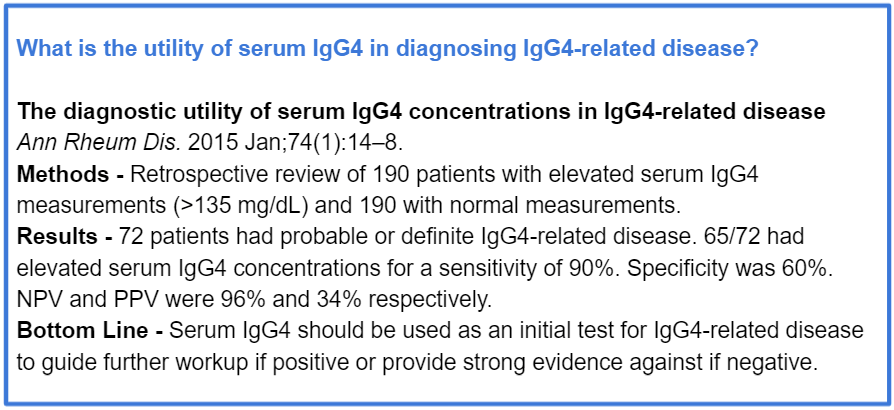
Discussion #3 @29:32 – Differential for elevated IgG4 beyond IgG4-related disease1,2
- Respiratory
- Bronchiectasis, chronic rhinosinusitis, asthma, idiopathic pulmonary fibrosis, sarcoidosis
- Repeated infections
- Autoimmune
- SLE, Sjogren syndrome, systemic sclerosis, rheumatoid arthritis, vasculitis
- GI
- Primary sclerosing cholangitis, biliary stricture or stone, pancreatitis, cirrhosis
- Cancer
More information
- Investigations
- Bloodwork
- Creatinine 100 µmol/L -> 130 µmol/L 2 weeks later, eGFR 60 -> 40 2 weeks later
- Lipase 30 IU/L
- IgE 3200 IU/mL
- C3 low, C4 unmeasurably low
- CRP normal
- Urine
- Protein 5+, hgb present
- Bloodwork
Discussion #4 @32:27 – IgE and asking Google for help
More information
- Investigations
- Renal biopsy
- Diffuse diabetic nephropathy
- Moderate involvement by plasma cell rich tubulointerstitial inflammation consistent with IgG4 renal disease
Discussion #5 @42:04 – What is IgG4-related disease?3,4
- Immune-mediated fibroinflammatory disease
- Epidemiology
- Majority (62-83%) are men and older than 50yrs of age
- Clinical features
- Presentation of subacute and diagnosis often incidental
- Patients may have disease confined to single organ or involvement of multiple organs
- Pancreas – Autoimmune pancreatitis. Imaging may show diffuse or segmental enlargement (“sausage-shaped pancreas”) surrounded by peripheral rim of low attenuation with pancreatic duct narrowing
- Eyes – Pain, peri-ocular tissue swelling, tumefactive lesions of the orbit or peri-orbital tissues
- Ears, nose, sinuses – Allergic features are common, including atopy, eczema, asthma, peripheral blood eosinophilia, sinusitis
- Salivary gland – Submandibular and/or parotid gland enlargement
- Meninges – Headache, radiculopathy, cranial nerve palsy, cord compression, mass lesions
- Pituitary – Hormone deficiencies, headache, visual disturbance
- Lymph nodes – Generalized or localized lymphadenopathy
- Thyroid gland – Hypothyroidism, thyroid enlargement
- Lungs – Cough, hemoptysis, pleural effusion, dyspnea
- Aorta – Aortitis, dissection
- Retroperitoneum – Backache, abdominal pain, lower extremity edema, hydronephrosis depending on extent of fibrosis
- Kidney – Proteinuria, hematuria, decreased kidney function. Typically involves tubulointerstitial nephritis
- Biliary tree – Obstructive jaundice associated with autoimmune pancreatitis
- Liver – Mass lesions, obstructive jaundice
- Phenotypes
- Group 1 – pancreatohepatobiliary disease
- Group 2 – retroperitoneal fibrosis and aortitis
- Group 3 – head and neck limited disease
- Group 4 – Mikulicz syndrome, systemic involvement
- Diagnosis
- Elevated tissue concentrations of IgG4 in tissue and serum is helpful
- Ultimately based on histopathology
- Dense lymphoplasmacytic infiltrate
- Storiform fibrosis
- Obliterative phlebitis
- Treatment
- Urgency and indications for systemic treatment depend on organs affected and degree of severity
- First line therapy is glucocorticoids
- Gucocorticoid-sparing agents or maintenance drugs include azathioprine, mycophenolate mofetil, and methotrexate
- Rituximab can be used, primarily for recurrent or refractory disease

- Ebbo M, Grados A, Bernit E, Vély F, Boucraut J, Harlé J-R, et al. Pathologies Associated with Serum IgG4 Elevation. Int J Rheumatol. 2012;2012:602809.
- Ryu JH, Horie R, Sekiguchi H, Peikert T, Yi ES. Spectrum of Disorders Associated with Elevated Serum IgG4 Levels Encountered in Clinical Practice. Int J Rheumatol. 2012 May 27;2012:e232960.
- Stone JH, Zen Y, Deshpande V. IgG4-Related Disease. N Engl J Med. 2012 Feb 9;366(6):539–51.
- Wallace ZS, Zhang Y, Perugino CA, Naden R, Choi HK, Stone JH, et al. Clinical phenotypes of IgG4-related disease: an analysis of two international cross-sectional cohorts. Ann Rheum Dis. 2019 Mar;78(3):406–12.
