Today we explore the case of a healthy man whose symptoms of headache and dyspnea at first glance seem to be obviously explained, until things don’t go quite as expected. Stay tuned as we explore the causes for our patients presentation and how that changes as the clinical course progresses.
ID –
66 yo Caucasian male presenting with 3 days of headache, transient confusion, and dyspnea
HPI –
Apr. 17 – Son-in-law admitted to SPH ICU for meningitis secondary to group C strep complicated by endocarditis. Patient was started on cephalexin for prophylaxis
Apr. 19 – Patient flew to Vancouver to visit son-in-law, asymptomatic at the time
Apr. 22 – Worsening headache, pain with chewing. Saw neurologist who increased pregabalin to 150mg BID as thought to be from trigeminal neuralgia
Apr. 23 – Worsening dyspnea, particularly with exertion
Apr. 24 – Dyspnea continues to worsen, fatigue, some unintelligible speech, gait instability
Apr. 25 – Difficult to rouse, 8/10 frontotemporal and constant headache, neck stiffness, photophobia, fluctuating level of consciousness with moments of confusion and speech change, fever.
Presented to SPH ED.
At few days prior to hospitalization, family noted rash on palms and soles
PMHx –
Trigeminal neuralgia diagnosed 1 mo ago
Parkinson’s disease diagnosed 5 yrs ago
Medications –
Cephalexin 500mg QID started 1 wk ago for strep prophylaxis
Levodopa/carbidopa CR 200mg/50mg 5x per day
Levodopa/carbidopa IR 100mg/25mg QID
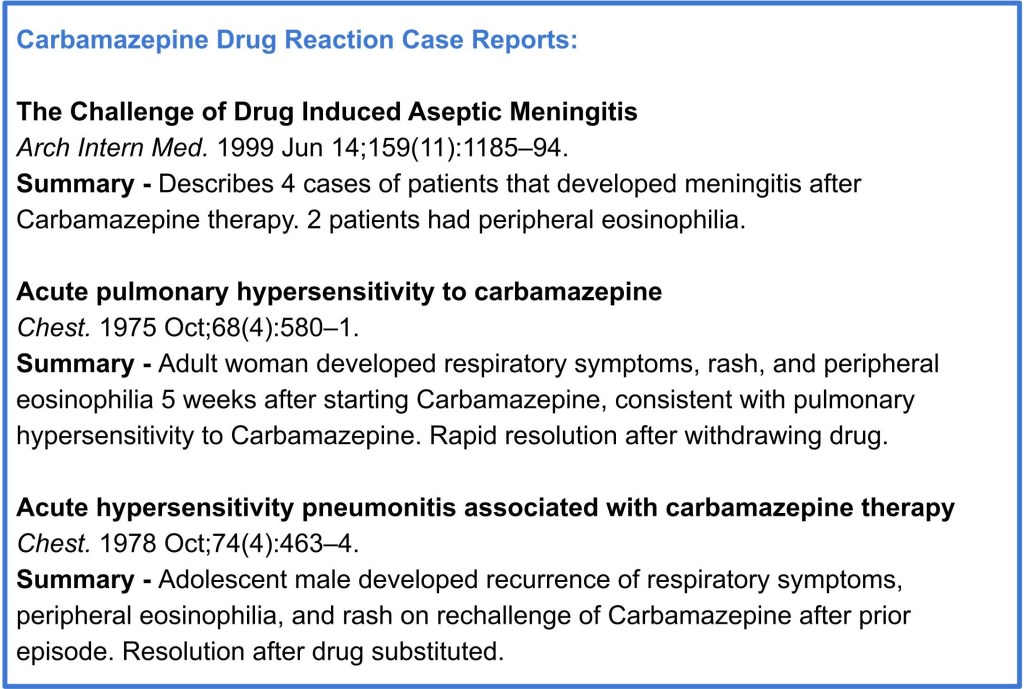
Carbamazepine 600mg BID started 3 wks ago
Pregabalin 150mg BID started 3 wks ago with recent dose increase
Social Hx –
Lives in Whitehorse, Yukon with daughter, son-in-law, and pet dog
Works in community reclamation projects including old mine sites, residential schools. Potential exposures to asbestos, mouse trapping, lead paint, animals, etc.
Most recent travel to Norway 1mo ago, encountered reindeer
30 pack year history of smoking, no recreational drugs or alcohol
Allergies –
No known drug allergies
Initial Exam
- BP 119/56, HR 93, RR 20, 92% O2 sat on room air, Temp 38.1 ℃
- Alert and oriented, appears uncomfortable
- Skin – Blanching, macular, non-pruritic, erythematous rash on posterior ankles, dorsum of left foot, and abdomen. No stigmata of endocarditis
- Respiratory – Bibasilar crackles on inspiration
- Cardiac and GI – unremarkable
- Head and neck – slight nuchal rigidity, no cervical lymphadenopathy
- Neurologic – 4+ bilateral patellar reflexes with clonus, slight tremor, negative Brudzinski and Kernig signs, otherwise unremarkable
Initial Investigations
- Blood
- WBC 16.3 x 109/L (normal 3.5 – 10.5 x 109/L), neutrophil count 12.3 x 109/L (normal 2.0 – 7.5 x 109/L)
- Hgb 129 g/L (normal 125 – 170 g/L)
- Plt 272 x 109/L (normal 130 – 380 x 109/L)
- INR and PTT normal
- Electrolytes, extended electrolytes, urea, creatinine, glucose – normal
- Infectious
- Influenza swab – negative
- Blood cultures – pending
- ECG – sinus rhythm, QTc 480ms
- Imaging
- CXR – minor fine reticular lines at costophrenic angles bilaterally, consistent with fibrosis or emphysematous change
- CT head – nil acute
- CT angio chest – no PE, extensive airway inflammation with patchy ground glass nodularity diffusely in sub-pleural distribution. Bronchitis and bronchiolitis, likely infectious etiology. Interlobular septal thickening most pronounced in lung bases. Mild bilateral hilar lymphadenopathy
- Procedures
- Lumbar puncture – WBC count 50 cells/µL, 63% neutrophils, 30% lymphocytes, 6% monocytes, 1% eosinophils, RBC count 1840 cells/mm3, no organisms on gram stain, gluc 4.4 mmol/L, protein 0.35 g/L, opening pressure not recorded
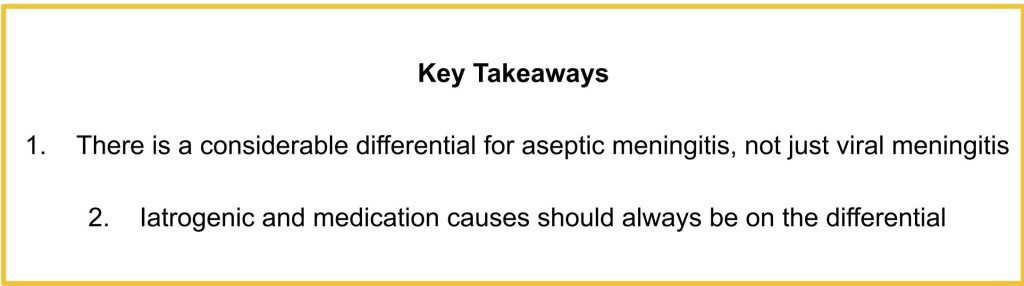
Discussion #1 @6:25 – Initial broad differential
| Differential | Factors For | Factors Against |
| 1. Viral meningoencephalitis – Enterovirus* – Herpes simplex* – Varicella zoster – HIV | – Abnormal CSF – Meningismus – Acute illness progression – Could involve lungs – Rash on palms and soles could be secondary to coxsackievirus | |
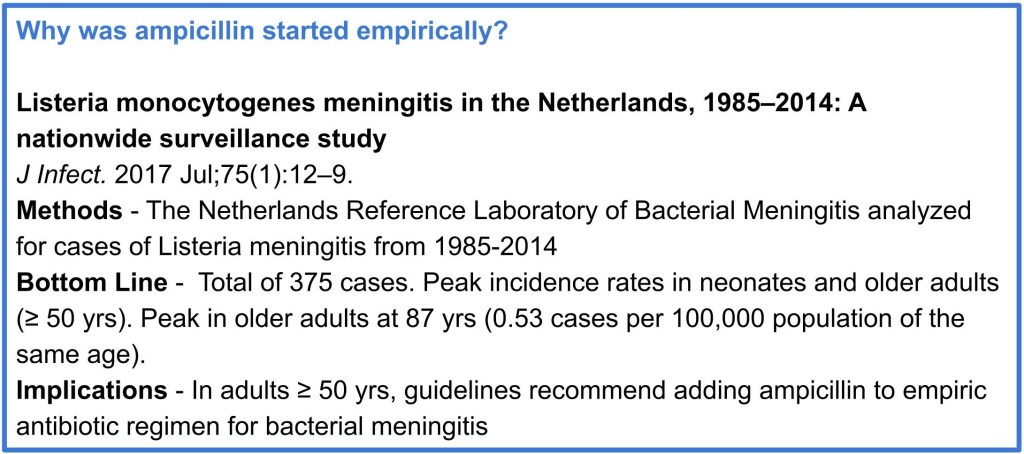
| 2. Bacterial meningitis – Streptococcus pneumoniae* – Nisseria meningitidis* – Haemophilus influenzae – Listeria monocytogenes – Neurosyphilis – Lyme disease – Q fever – Mycobacterium – Invasive group C strep | – Abnormal CSF – Meningismus – Acute illness progression – Could involve lungs – Son-in-law recent episode of bacterial meningitis – Rash on palms and soles could be secondary to syphlis – Antibiotic prophylaxis could be confounder – TB risk factor – exposure to indigenous communities – Q fever risk factor – contact with animals | – CSF not classic but does not rule out |
| 3. Fungal meningitis – Cryptococcus – Coccidioides | – Meningismus – Abnormal CSF – Could involve lungs | – No evidence of immunocompromise – Acute illness progression |
| 4. Inflammatory – Neurosarcoidosis – SLE | – Abnormal CSF – Could involve lungs | – Acute illness progression |
| 5. Drug-induced meningitis | – Abnormal CSF – In last month, cephalexin, carbamazepine, pregabalin started – Could involve lungs – Could cause drug rash | – Diagnosis of exclusion, need to rule out other causes |
More information
- Investigations
- Infectious
- Blood, CSF, sputum cultures – negative
- Respiratory virus panel – negative
- HIV – negative
- Cryptococcus antigen – negative
- HSV PCR, VZV PCR on CSF – negative
- Acid fast stain – pending
- Hantavirus PCR – pending
- Coxiella burnetti serology – pending
- Legionella urinary antigen – pending
- Rheumatologic
- ANA, ANCA – negative
- Hematologic
- Peripheral eosinophil count – 0.9 x109 cells/L
- Infectious
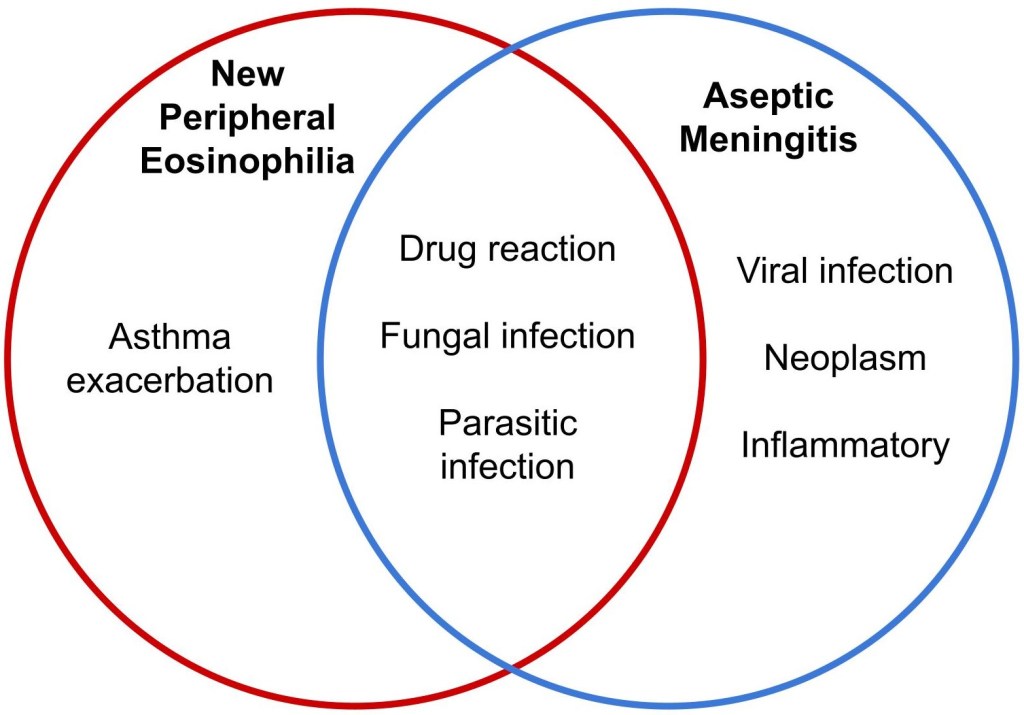
Discussion #2 @21:06 – Narrowing the differential and considering new eosinophilia
More information
- Investigations
- Imaging
- MRI brain – minimal meningeal enhancement, no other intracranial abnormalities
- Procedures
- Bronchoscopy –
- BAL – 33% monocytes, 19% eosinophils, 19% neutrophils, 3% basophils, 26% lymphocytes. Atypical cells, query reactive vs malignant
- Cytology and cytometry – negative for malignancy
- Gram stain and culture – scant candida growth
- No biopsy done
- Bronchoscopy –
- Infectious
- Fungal culture on CSF – negative
- Stool ova and parasites – negative
- Strongyloides serology – negative
- Mycobacterial culture and AFB – negative
- Legionella urine antigen – pending
- Hantavirus PCR – pending
- Coxiella burnetti serology – pending
- Hematologic
- Peripheral eosinophil count 1.1 x 109 cells/L
- Imaging
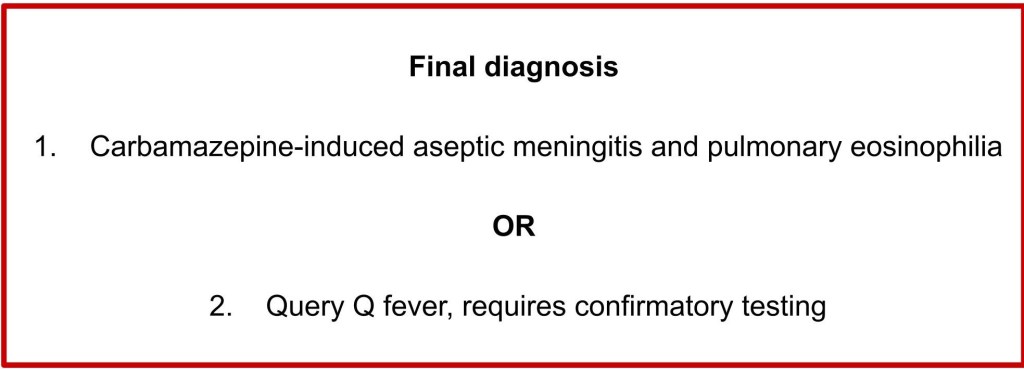
Discussion #3 @30:55 – Final differential
| Differential | Factors For | Factors Against |
| 1. Drug reaction – Most likely Carbamazepine | – Abnormal CSF – In last month, cephalexin, carbamazepine, pregabalin started – Could involve lungs – Could cause drug rash – Could cause eosinophilia – Rapid improvement following stopping Carbamazepine | |
| 2. Viral meningoencephalitis – Hantavirus, coxiella burnetti serology pending | – Abnormal CSF – Meningismus – Acute illness progression – Could involve lungs | – No virus identified yet – Would not explain eosinophilia |
| 3. Bacterial meningitis – Coxiella burnetti serology pending | – Meningismus – Acute illness progression – Could involve lungs – Improvement could be delayed response to previous antibiotics | – No bacteria identified yet – Would not explain eosinophilia |
More information
- Investigations
- 10 days post-discharge – Coxiella burnetti IgM – positive, IgG – negative